Retake
V5) Dyspnea and chest pain after car travel
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Analyze the role of consulting diagnostic radiologists in evaluating a patient with dyspnea.
- Review the DDx considerations in a patient with dyspnea.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with dyspnea.
History
An 80-year-old male with a history of AV block requiring a pacemaker is brought to the ED with acute onset shortness of breath, lightheadedness, and chest pain. The chest pain worsens upon taking deep breaths. The patient has been mostly sedentary following surgery for a right bimalleolar ankle fracture, which is now in a cast. He also recently traveled 8 hours by car for a family trip. The patient does not take any anticoagulants, denies bleeding disorders, has no recent major brain surgery, and denies any other past medical history.
Physical Exam
BP: 75/50, HR 110, RR 30, Temp 37ºC, O2 saturation 88%.
Lung exam: Bilaterally clear to auscultation with no crackles, wheezing, or rhonchi.
Cardiovascular exam: Tachycardic, regular rhythm, normal S1 and S2 sounds, swelling and erythema of the right lower extremity.
Labs
D-dimer: 950 ng/mL (normal < 500 ng/mL).
Troponin I: <0.01 ng/mL.
EKG: Tachycardic, no ST changes.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient most likely has a massive pulmonary embolism, given the sudden onset of pleuritic chest pain, shortness of breath, and hemodynamic instability (manifested as hypotension, tachycardia, and tachypnea). Supporting laboratory findings include elevated D-dimer levels. Additionally, the patient has notable risk factors such as endothelial injury (due to recent lower extremity surgery) and venous stasis (resulting from immobilization due to casting and extended travel). The presence of swelling and erythema in the right lower extremity suggests that the pulmonary embolism may be secondary to a deep venous thrombosis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This hemodynamically unstable patient requires emergent workup.
First Imaging Study
What is the first imaging study you will order?
The CT angiography is considered the most appropriate initial imaging modality to detect any filling defects in the pulmonary vasculature, which may indicate an embolus.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
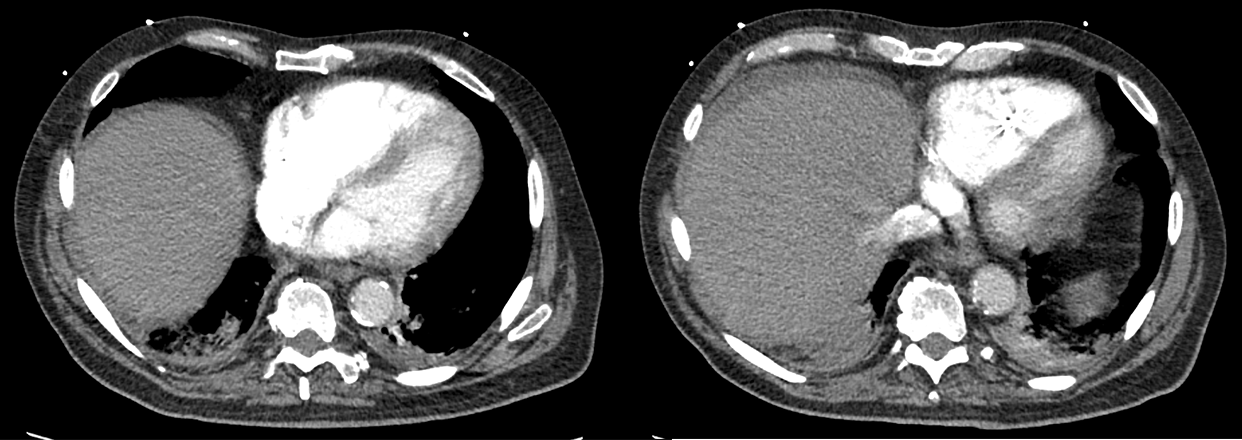
Chest CT angiography
Is there a filling defect in the pulmonary vasculature?
There is a saddle pulmonary embolus straddling the bilateral main pulmonary arteries.
Is there evidence of right heart strain?
There is right heart strain, as evidenced by the enlarged right ventricle, interventricular septum flattening/bowing, and reflux of contrast into the inferior vena cava (IVC).
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is needed as the diagnosis is confirmed with CTA.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
Obstructive shock is a type of shock caused by a physical obstruction in the cardiovascular system. In this case, it is secondary to a pulmonary embolism. Other potential causes include tension pneumothorax, cardiac tamponade, or superior vena cava syndrome.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient requires emergent management.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is an 80-year-old male presenting with a saddle pulmonary embolism. To address this, it is recommended to obtain IV access and administer vasopressors and oxygen therapy. Systemic thrombolytic therapy should be initiated followed by anticoagulation, provided that the patient has no contraindications.
To prevent recurrence, a transition to long-term anticoagulation such as a DOAC or warfarin is suggested. It is also necessary to conduct a lower extremity ultrasound to further evaluate the presence and extent of DVTs.
Lessons Learned:
- Pulmonary embolism (PE) is a serious condition with various risk factors that can lead to blood clot formation in the pulmonary vasculature. Major risk factors include immobility (after prolonged travel or surgery), inherited hypercoagulability disorders, recent surgery, estrogen therapy, trauma, malignancy, and pregnancy. These risk factors are encompassed by Virchow’s triad, which describes the pathophysiology of clot formation in the vascular system: endothelial injury, hypercoagulability, and venous stasis.
- CTA is the imaging modality of choice for diagnosing PE, as it can reveal filling defects in the pulmonary vasculature. A serum D-dimer test is highly sensitive for detecting PE, although it lacks specificity since it can also be elevated in other conditions that cause fibrin degradation.
- PE should be considered in all patients with acute dyspnea, as symptoms such as shortness of breath, tachycardia, and chest pain are nonspecific.
- Treatment of PE generally involves oxygen supplementation and anticoagulation. However, high-risk PEs, such as a saddle PE leading to obstructive shock, may require aggressive management, which can include thrombolysis, surgical embolectomy, catheter-directed thrombolysis, or catheter-directed thrombectomy. Early recognition and prompt treatment are crucial for improving patient outcomes.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}